SICOT Global Network for Electronic Learning - SIGNEL
Case of the Month
December 2014
Authors: Syah Bahari & John McKennaKPJ Healthcare University College, Nilai, Malaysia & Sport Surgery Clinic, Santry, Dublin, Ireland
History
A 22-year-old male presented with one week's history of left ankle injury during a soccer match. According to the patient, he was tackled during the match but was able to continue playing afterwards. However, he noted that the left ankle was quite swollen after the match and was progressively getting worse. He was given anti-inflammatory medication by his team doctor, which eased the pain. He was advised to keep the leg elevated and applied an ice pack. The swelling has improved over time, but he is still complaining of pain on weight bearing. On examination, it was a closed injury. There was soft tissue swelling around the ankle joint with effusion. Alignment of the foot and ankle was satisfactory on weight bearing. The ankle range of motion was not significantly limited when compared during active and passive motions. The neurovascular examination was satisfactory.
A radiograph of the foot was performed and showed a cyst on the medial aspect of the distal tibia. A CT scan was subsequently performed for further evaluation.

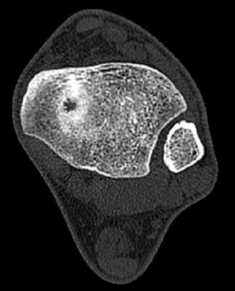
Q. What are your thoughts on the findings of the CT scan?
The CT scan showed erosive lesion with sclerotic margin. The lesion is also in communication with the ankle joint.
Q. What is the next step in your management plan?
Treatment
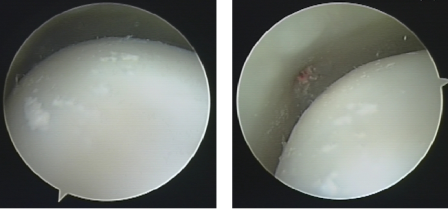
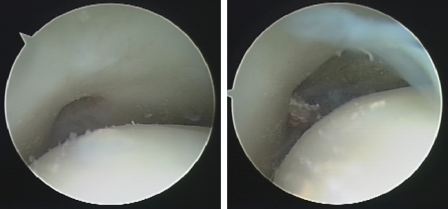
The patient underwent ankle arthroscopy. It was noted there was white chalky particulate debris in the joint, which arises from the lesion that was communicating intra-articularly. The lesion was debrided and irrigation of the ankle joint was performed. Joint aspiration and synovial biopsy from the lesion showed uric acid crystal formation suggestive of acute gouty arthritis. Patient was started on Allupurinol in view of the diagnosis. Patient was clinically well at 3 months' follow-up.
The CT scan showed erosive lesion with sclerotic margin. The lesion is also in communication with the ankle joint.
Q. What is the next step in your management plan?
- Further investigation with MRI scan of ankle
- Open biopsy of the lesion
- Ankle arthroscopy for evaluation of the lesion
Treatment
The patient underwent ankle arthroscopy. It was noted there was white chalky particulate debris in the joint, which arises from the lesion that was communicating intra-articularly. The lesion was debrided and irrigation of the ankle joint was performed. Joint aspiration and synovial biopsy from the lesion showed uric acid crystal formation suggestive of acute gouty arthritis. Patient was started on Allupurinol in view of the diagnosis. Patient was clinically well at 3 months' follow-up.
Discussion
Patients with an acute gouty arthritis are classically present with acute painful 1st MTP joint also known as podagra. However, acute gouty arthritis has been reported to present as acute joint pain and swelling other than the 1st MTP joint such as ankle, knee, elbow and wrist [1,2].
Radiographic changes are not the hallmark of acute gouty arthritis at the early stage of the disease. Erosive lesion with or without involvement of the joint has been described but these changes are often seen as the condition progresses [2].
There was a previous case of cystic lesion involving the talus, which was diagnosed histologically as tophaceous gout [3]. The authors also noted the chalk-like material during arthroscopy. Similarly, the patient was treated with antihyperuricaemic medication with satisfactory outcome.
References
Patients with an acute gouty arthritis are classically present with acute painful 1st MTP joint also known as podagra. However, acute gouty arthritis has been reported to present as acute joint pain and swelling other than the 1st MTP joint such as ankle, knee, elbow and wrist [1,2].
Radiographic changes are not the hallmark of acute gouty arthritis at the early stage of the disease. Erosive lesion with or without involvement of the joint has been described but these changes are often seen as the condition progresses [2].
There was a previous case of cystic lesion involving the talus, which was diagnosed histologically as tophaceous gout [3]. The authors also noted the chalk-like material during arthroscopy. Similarly, the patient was treated with antihyperuricaemic medication with satisfactory outcome.
References
- Nakayama DA, Bathelemy C, Carrera G et al. (1984) Topacheous gout: A clinical and radiographic assessment. Arthritis Rheum. 27:468-471
- Resnick D. (1996) Gouty arthritis. Bone and Joint Imaging. 2nd Edition. Philadelphia. WB Saunders Co. 395-408
- Raikin S, Cohn BT. (1997) Intraosseous gouty invasion of the talus. Foot Ankle Int. 18(7):439-42
 Â